| 2002 |

|
YEAR BOOK |
Health Research Board & Coombe Women's Hospital
|
Molecular biology of Kaposi's sarcoma
|
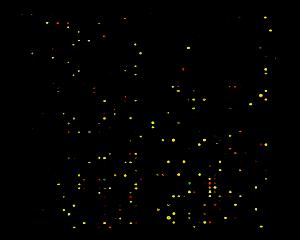
Part of this research involved taking skin biopsies of nodules of Kaposi's sarcoma kindly provided by five HIV positive Irish male patients and comparing them to normal skin biopsies from age and sex matched individuals, extracting genetic material (DNA and RNA) from each sample and analysing them using a research technique that has been recently developed called 'microarray technology' (see Figure). This allows one to study the genetic expression pattern of 2400 genes in the tumours and compare these patterns to those of the normal skin. Biopsies of Kaposi sarcoma lesions from 20 African patients were also assessed for the presence of the HHV 8 virus using antibodies against the virus.
Our results showed that 188/2400 genes were upregulated in the Kaposi tissue � i.e. 188/2400 genes in the Kaposi tissue showed increased activity, when compared to the normal skin. No genes were down regulated. The increased activity occurred in genes involved in control of the immune system, inflammation, connective tissue genes and genes involved in vessels and blood. The over expression of these gene groups could be partly explained by the nature of the components making up this tumour � i.e. the connective tissue, vessels, inflammatory cells, etc. The increased activity of genes involved in the immune system may reflect the fact the these tissues are from HIV positive patients, whose immune system is altered by the AIDS virus. It is possible that some of these genes are responsible for causing the Kaposi lesion, and further studies are needed to assess these.
HHV 8 was identified in all 20 African Kaposi lesions and the virus was localised to the spindle cells and vessel cells, suggesting the importance of this virus as a potential causitive factor in Kaposi's sarcoma.
This study gives a greater understanding of the molecular biology of Kaposi's sarcoma, and only through this understanding will we be able to attempt to develop new methods or improve current methods of treating this condition.
Contact: Dr Maria O'Donovan or Professor John J. O' Leary,
Department of Pathology,
Coombe Women's Hospital, Dublin 8;
E-mail: [email protected]